Authorized Representative Form California
Authorized Representative Form California - What is this form for? You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. This form is used to give permission to share personal information about you (the person who is seeking or. For questions, please call medi.
This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. For questions, please call medi. This form is used to give permission to share personal information about you (the person who is seeking or. What is this form for? You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you.
For questions, please call medi. You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. What is this form for? This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. This form is used to give permission to share personal information about you (the person who is seeking or.

How to an Authorized Representative for Your Loved One Your
This form is used to give permission to share personal information about you (the person who is seeking or. This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. For questions, please call medi. You have the right to authorize (give) a friend, family member, or other person you identify access.
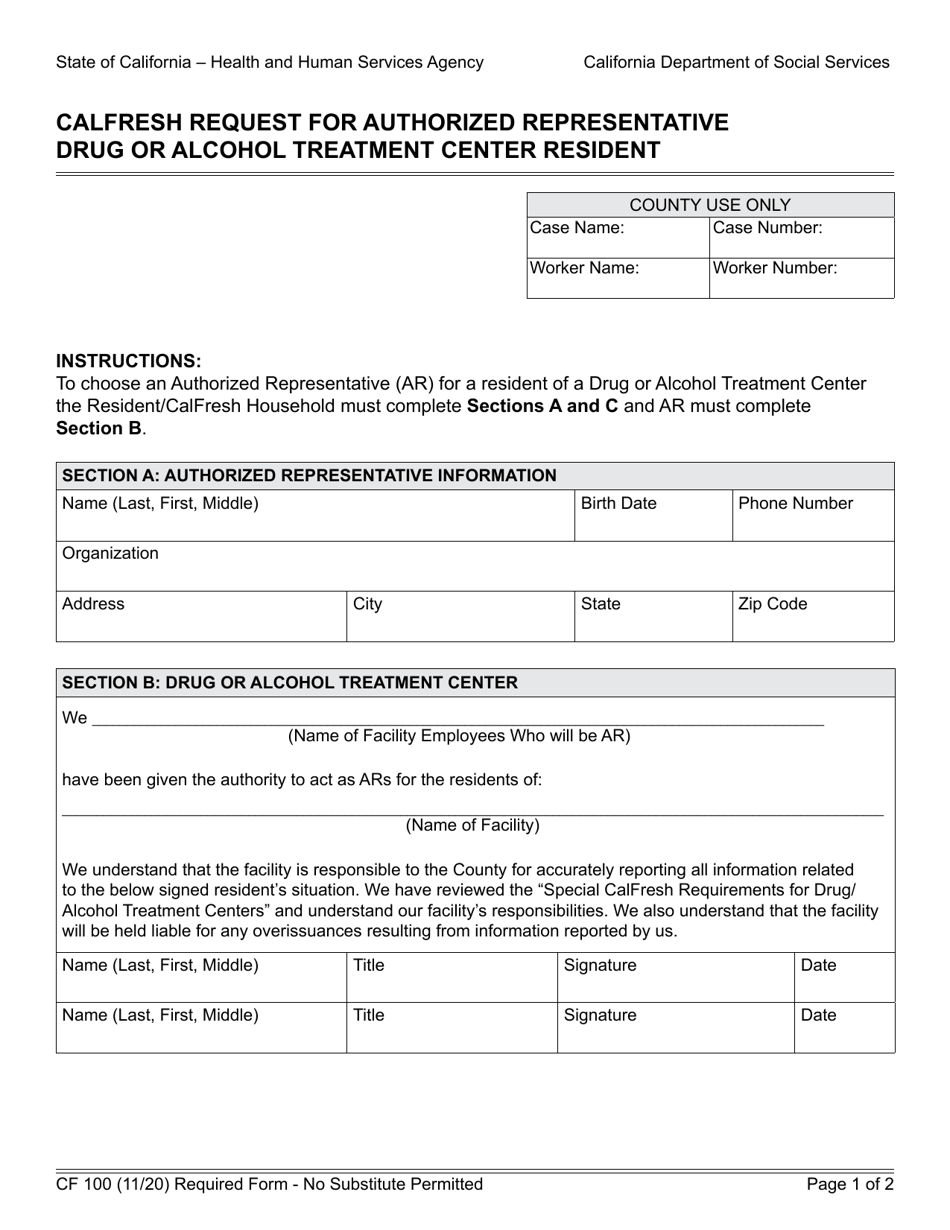
Form CF100 Fill Out, Sign Online and Download Fillable PDF
This form is used to give permission to share personal information about you (the person who is seeking or. What is this form for? You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. For questions, please call medi. This form allows you, as the ihss applicant/recipient.
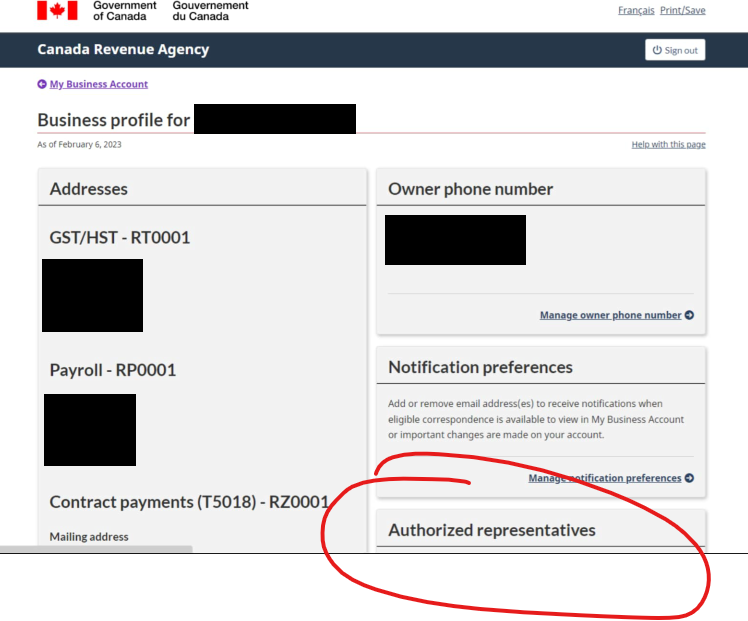
How to Authorize a Representative for your CRA Accounts Horizon CPAs
This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. This form is used to give permission to share personal information about you (the person who is seeking or. What is this form for? You have the right to authorize (give) a friend, family member, or other person you identify access.

Blank Authorized Representative Form Fill Out and Print PDFs
This form is used to give permission to share personal information about you (the person who is seeking or. What is this form for? You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. This form allows you, as the ihss applicant/recipient or their legal representative, to.
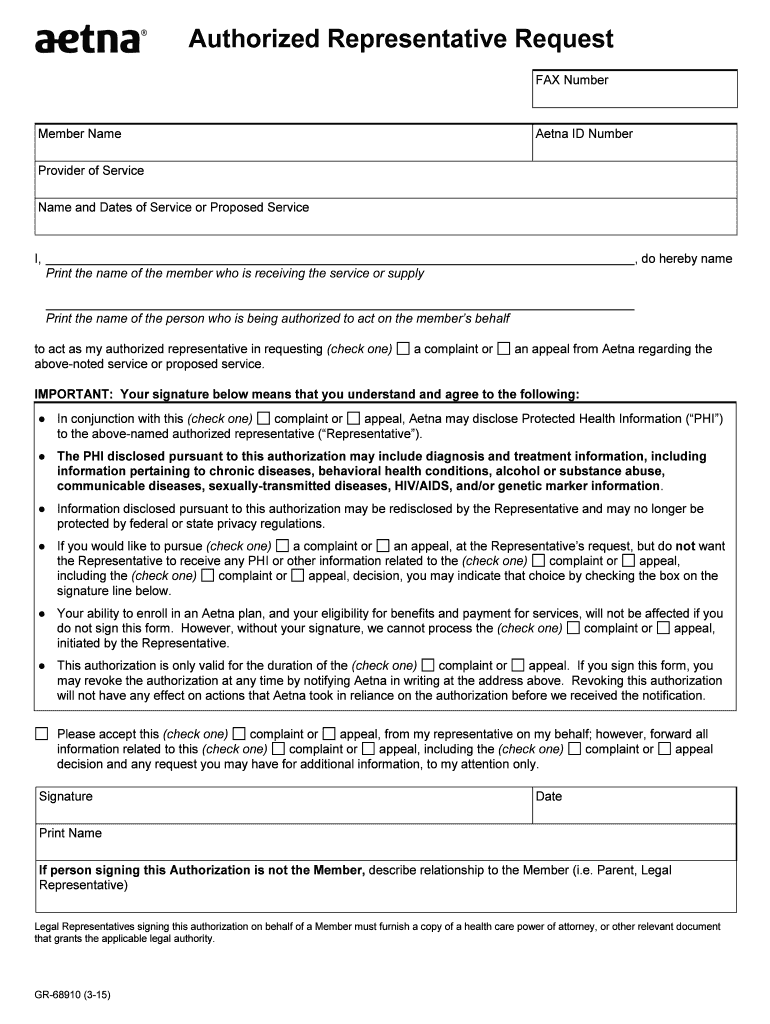
Aetna Authorized Representative Request 20152024 Form Fill Out and
This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. For questions, please call medi. This form is used to give permission to share personal information about you.
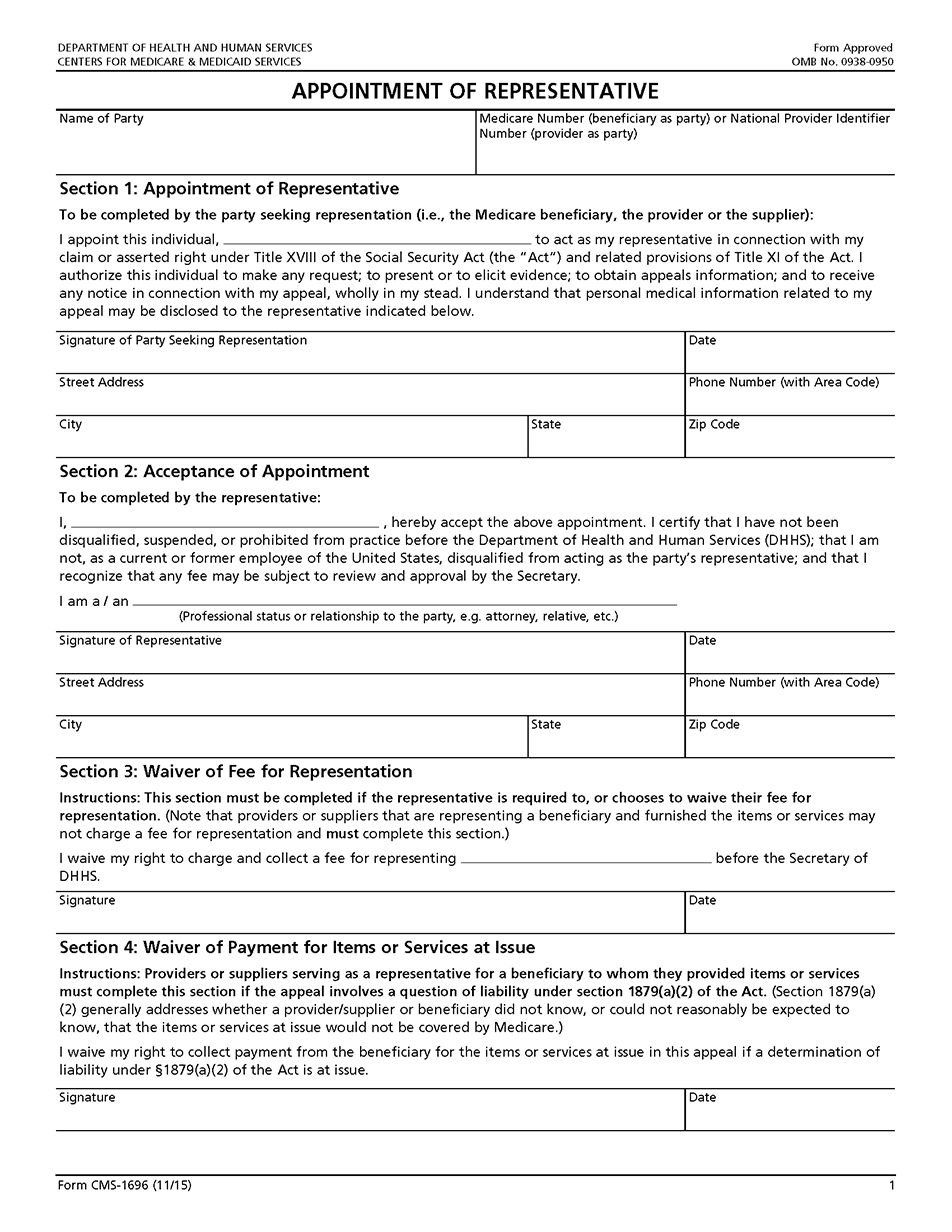
AOR Form Tutorial JE Part A Noridian
This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. For questions, please call medi. This form is used to give permission to share personal information about you (the person who is seeking or. What is this form for? You have the right to authorize (give) a friend, family member, or.
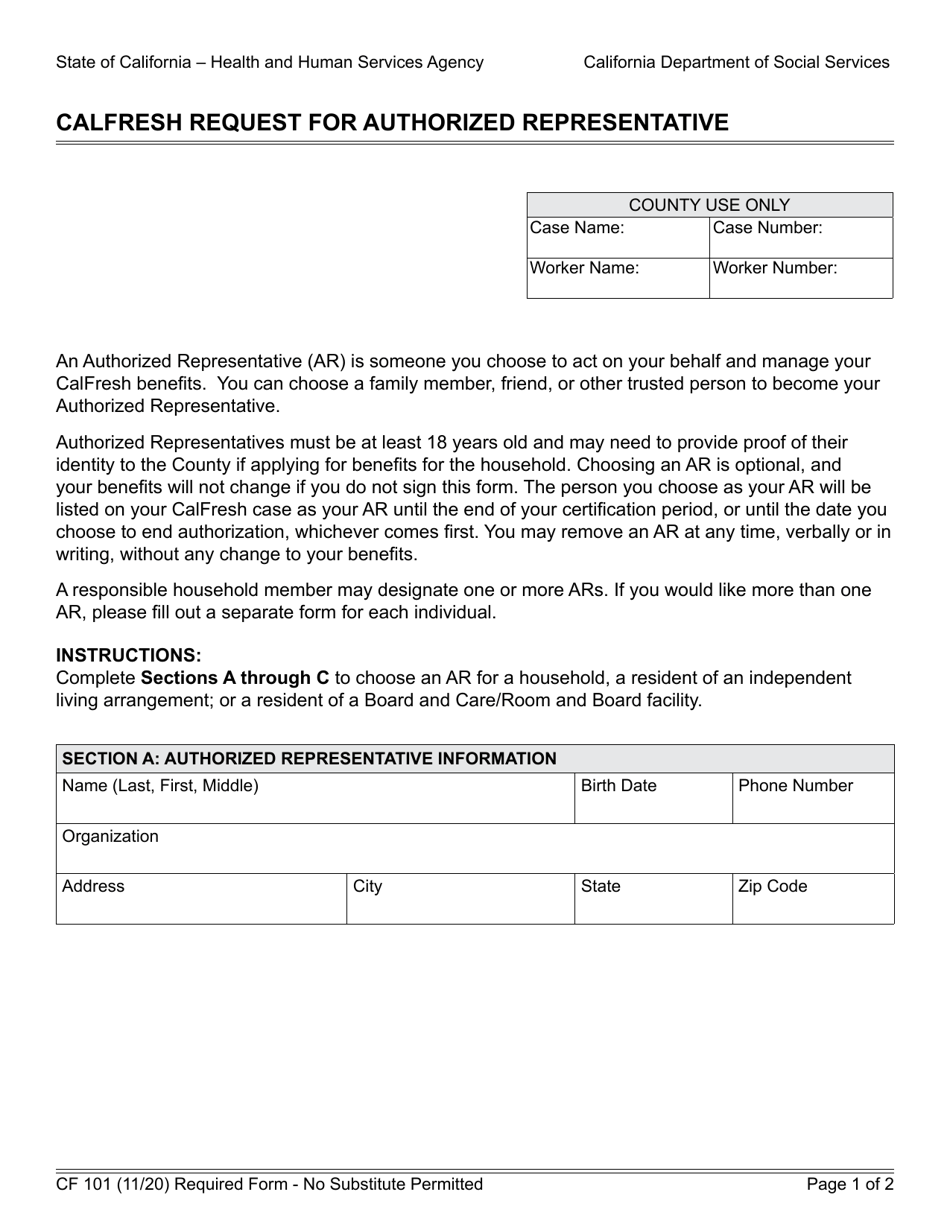
Form CF101 Fill Out, Sign Online and Download Fillable PDF
This form is used to give permission to share personal information about you (the person who is seeking or. You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. What is this form for? For questions, please call medi. This form allows you, as the ihss applicant/recipient.
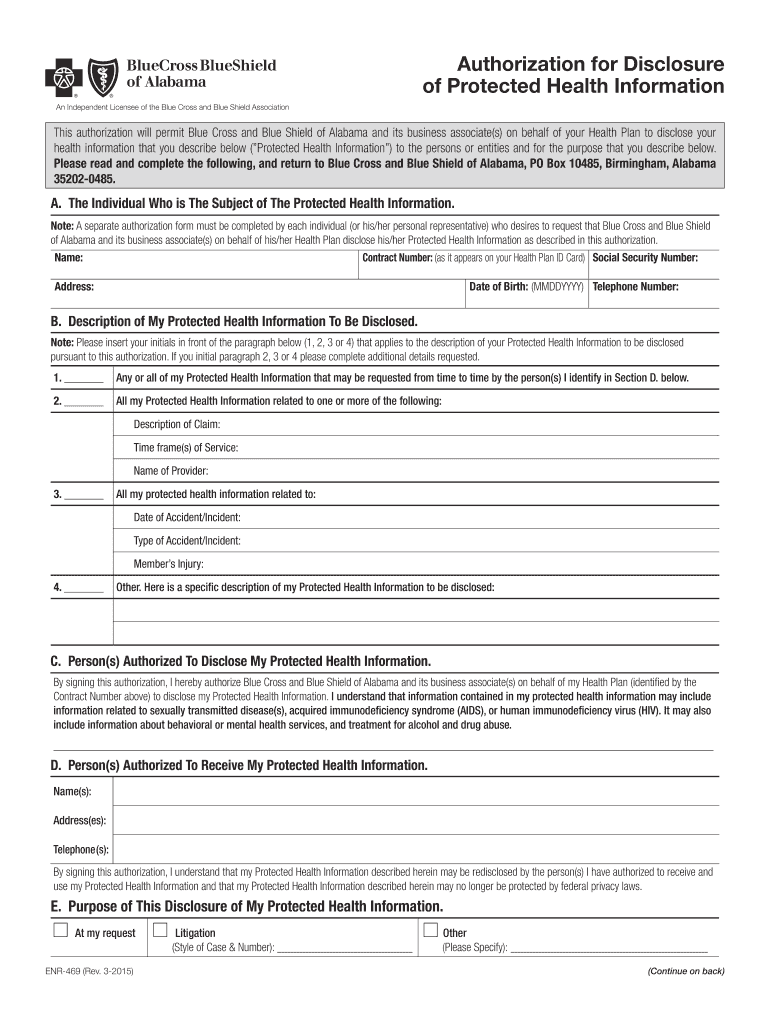
Printable Bcbs Application Form California Printable Forms Free Online
You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. This form is used to give permission to share personal information about you (the person who is seeking or. For questions, please call medi. What is this form for? This form allows you, as the ihss applicant/recipient.
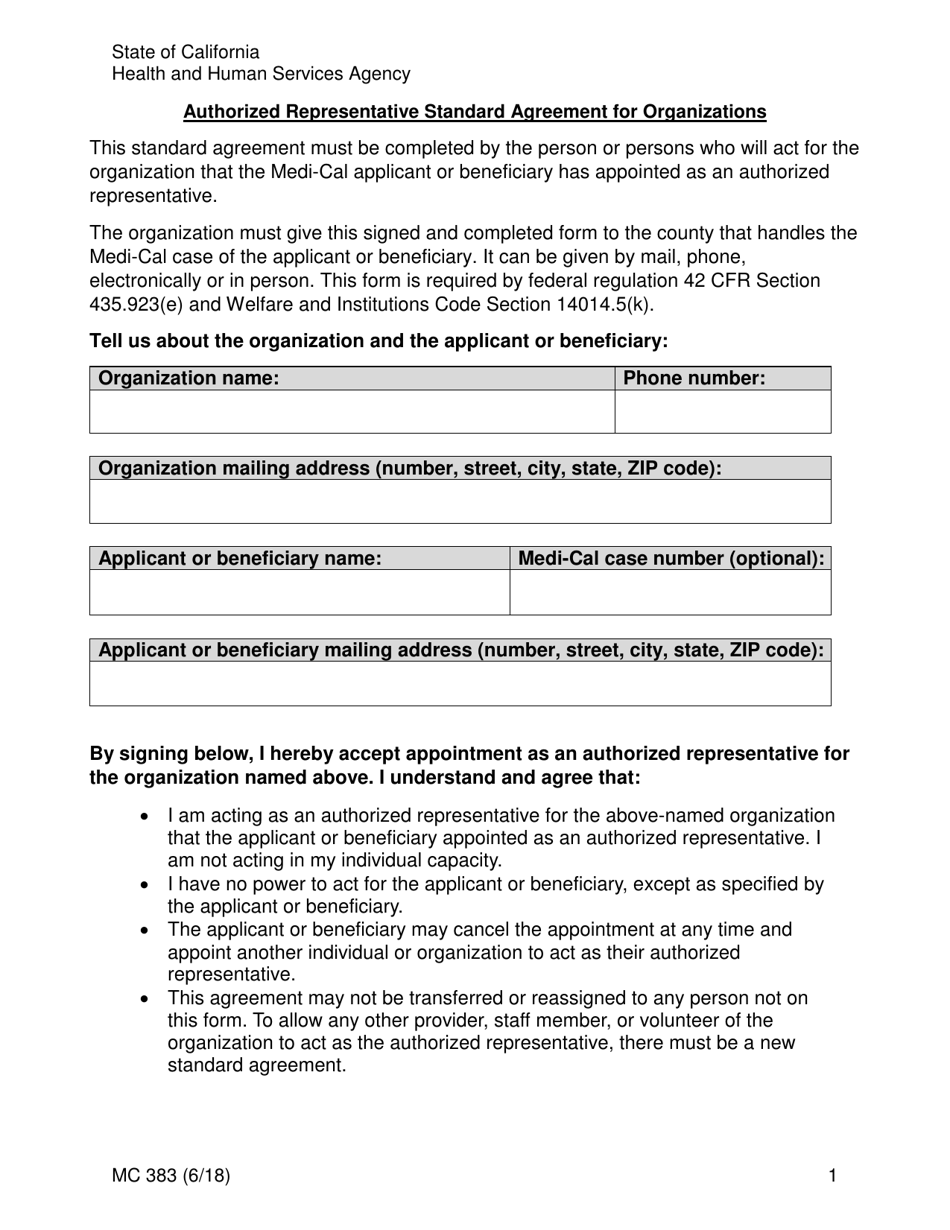
Form MC383 Fill Out, Sign Online and Download Fillable PDF
You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you. This form is used to give permission to share personal information about you (the person who is seeking or. For questions, please call medi. This form allows you, as the ihss applicant/recipient or their legal representative, to.
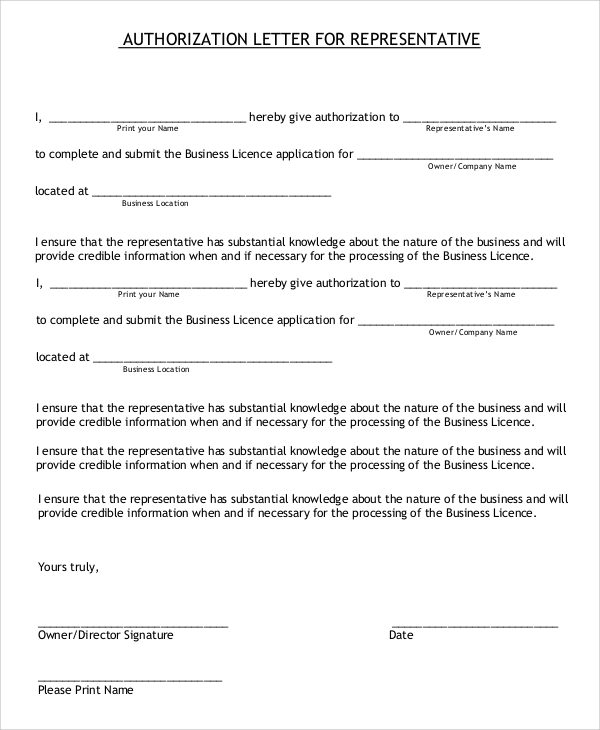
Authorization Letter For Representative
What is this form for? For questions, please call medi. This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. This form is used to give permission to share personal information about you (the person who is seeking or. You have the right to authorize (give) a friend, family member, or.
What Is This Form For?
For questions, please call medi. This form is used to give permission to share personal information about you (the person who is seeking or. This form allows you, as the ihss applicant/recipient or their legal representative, to choose an authorized representative for the. You have the right to authorize (give) a friend, family member, or other person you identify access to certain medical information about you.