Cobra Continuation Coverage Election Form
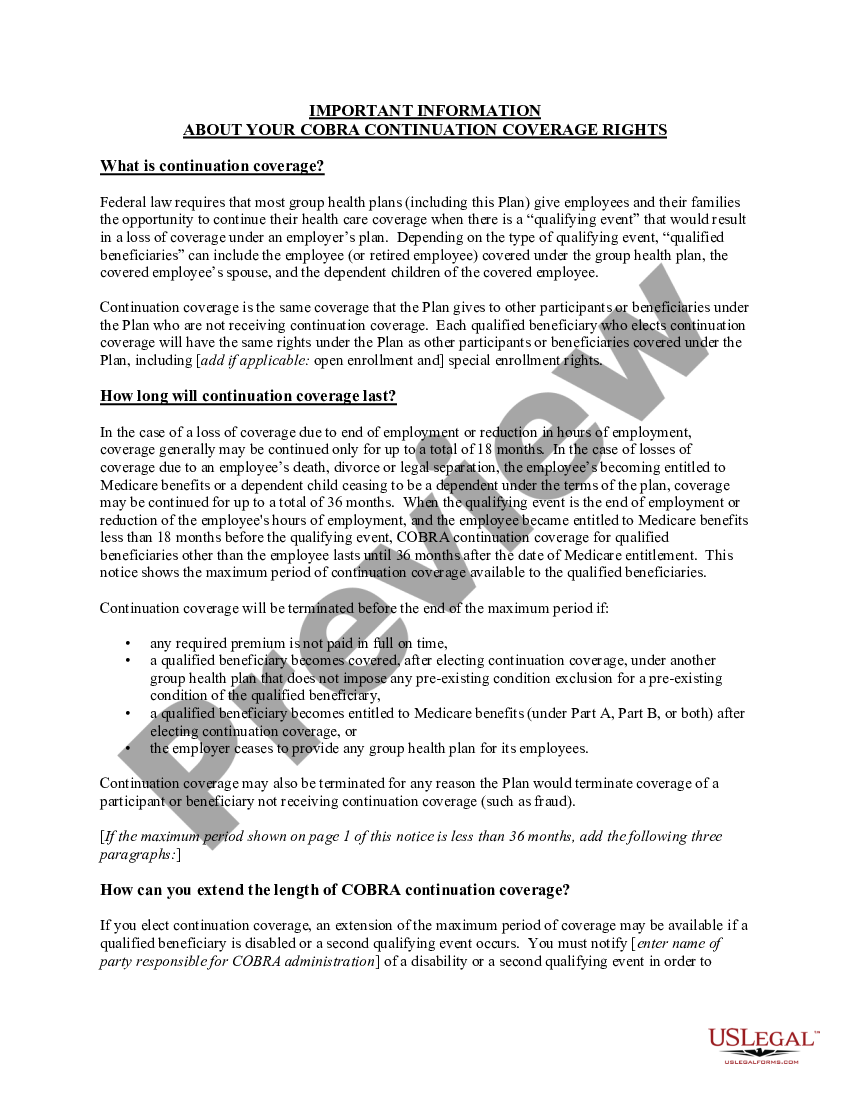
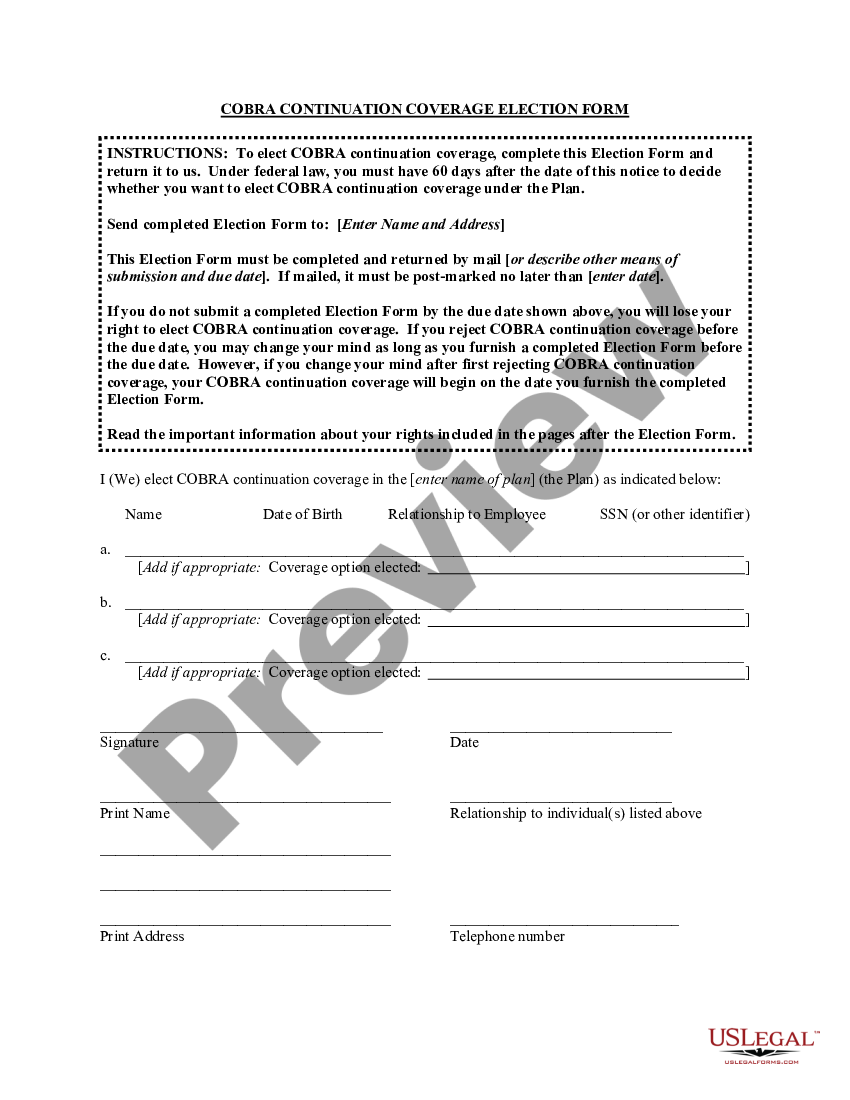
Cobra Continuation Coverage Election Form - Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us.
To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain.
Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain.
New Hampshire Model COBRA Continuation Coverage Election Notice Cobra
To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. If you choose to elect cobra continuation coverage, you should use the.
Model COBRA Continuation Coverage Election NoticeModel COBRA
If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed.
cobra notice Doc Template pdfFiller
To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Learn.
Montana Model COBRA Continuation Coverage Election Notice Cobra
Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. If you choose to elect cobra continuation coverage, you should use the election form provided later in this.
COBRA CONTINUATION WAIVER LETTER Form Fill Out and Sign Printable PDF
If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Learn.

Fillable Online COBRA Continuation Coverage Election Form (Outdated
Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Continuation coverage election form and first month’s premium payment (if electing cobra.
Puerto Rico Model COBRA Continuation Coverage Election Notice Cobra
Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for.
Montgomery Maryland Model COBRA Continuation Coverage Election Notice
Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for.
Maine COBRA Continuation Coverage Election Form Cobra Insurance US
To elect cobra continuation coverage, follow the instructions on the next page to complete the enclosed election form and submit it to us. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. Learn.
New Hampshire Model COBRA Continuation Coverage Election Notice Cobra
If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain. Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated.
To Elect Cobra Continuation Coverage, Follow The Instructions On The Next Page To Complete The Enclosed Election Form And Submit It To Us.
Continuation coverage election form and first month’s premium payment (if electing cobra coverage) to the designated employer. If you choose to elect cobra continuation coverage, you should use the election form provided later in this notice. Learn about your rights and responsibilities under cobra, a federal law that allows you to keep your health coverage for a limited time after certain.