New Patient Medical History Form
New Patient Medical History Form - New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the. No changes cancer arthritis depression/anxiety please list any. A comprehensive form to collect personal, medical, social and quality of life information from new patients. Have you ever been treated for any of the following medical conditions? A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation.
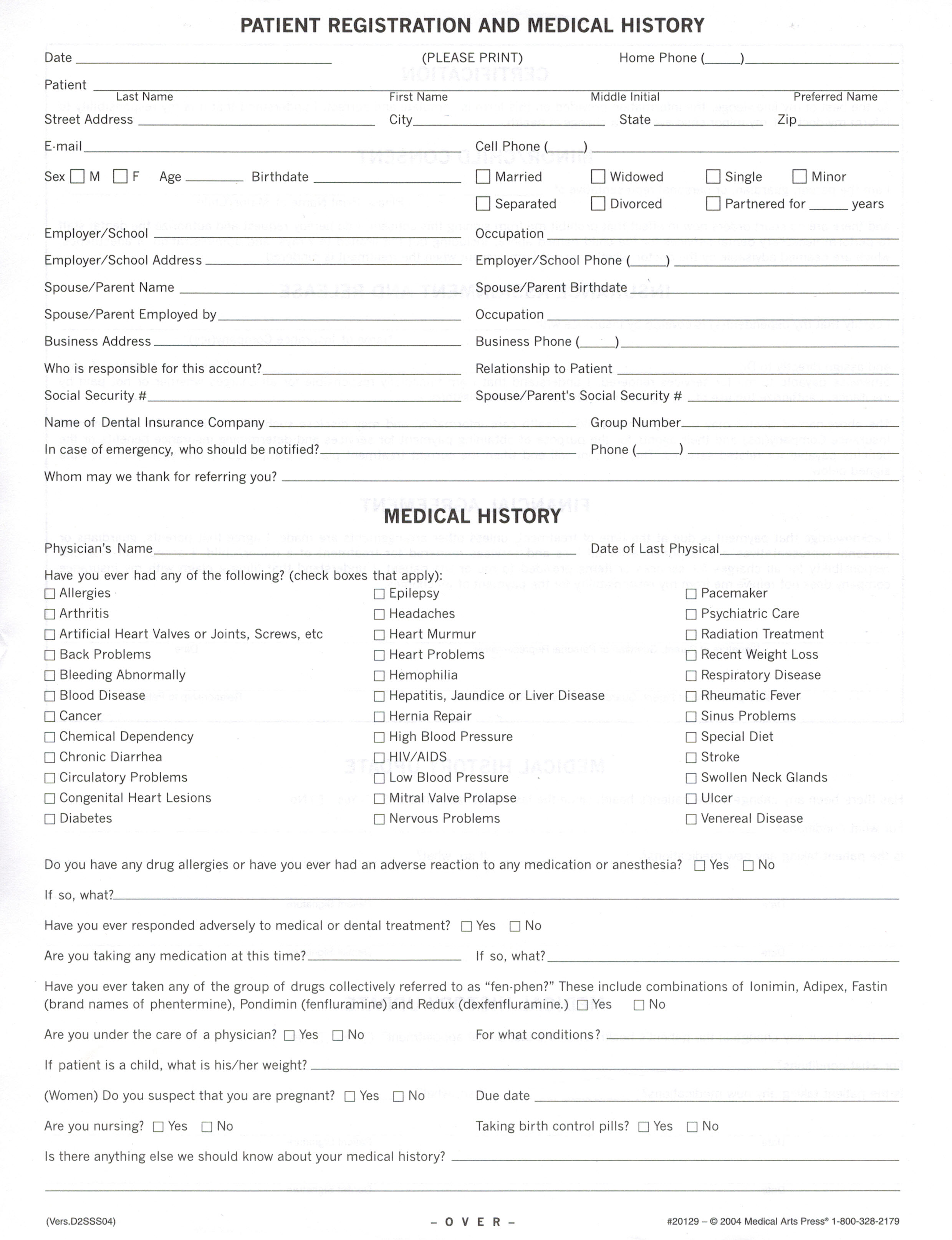
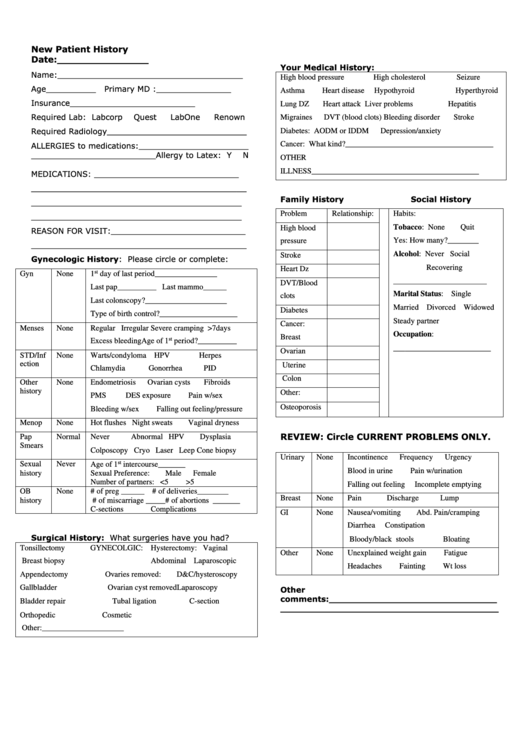
A comprehensive form to collect personal, medical, social and quality of life information from new patients. Have you ever been treated for any of the following medical conditions? New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. No changes cancer arthritis depression/anxiety please list any. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the.
A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. No changes cancer arthritis depression/anxiety please list any. The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: A comprehensive form to collect personal, medical, social and quality of life information from new patients. Have you ever been treated for any of the following medical conditions?
New Patient Health History Form Template Free Software and Shareware
No changes cancer arthritis depression/anxiety please list any. A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. Have you ever been treated for any of the following medical conditions? A comprehensive form to collect personal, medical, social and quality of life information from new patients. New patient medical history form name:_____ date of.
.png)
Medical History Form & Template Free PDF Download
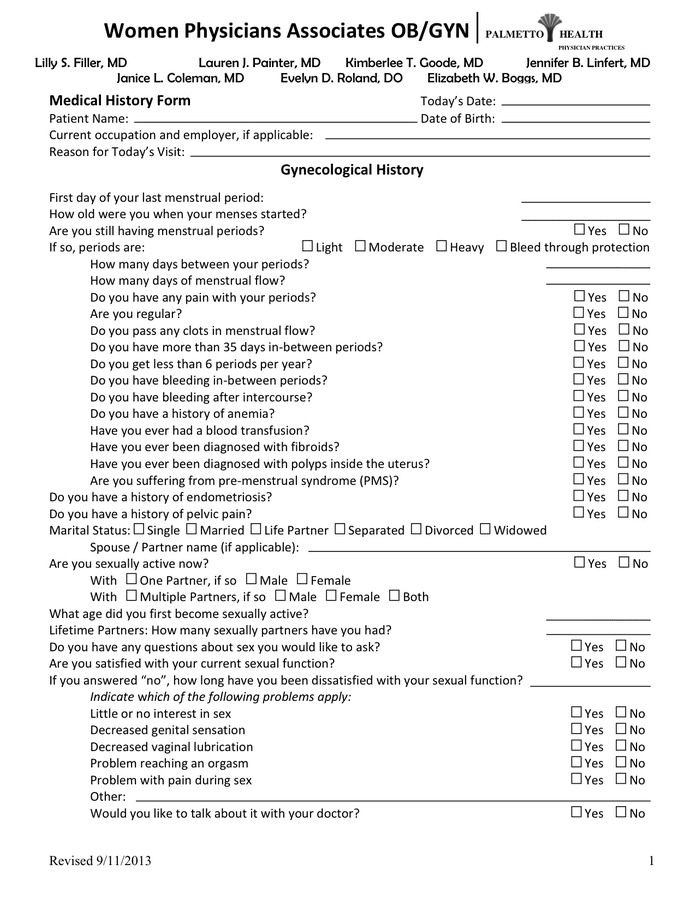
New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Have.
New Patient Medical History Form in Word and Pdf formats
A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the. Have you ever.
FREE 6+ Medical History Forms in PDF MS Word Excel
A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. Have you ever been treated for any of the following medical conditions? No changes cancer arthritis depression/anxiety please list any. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: A comprehensive form to collect personal,.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-01.jpg?w=395)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
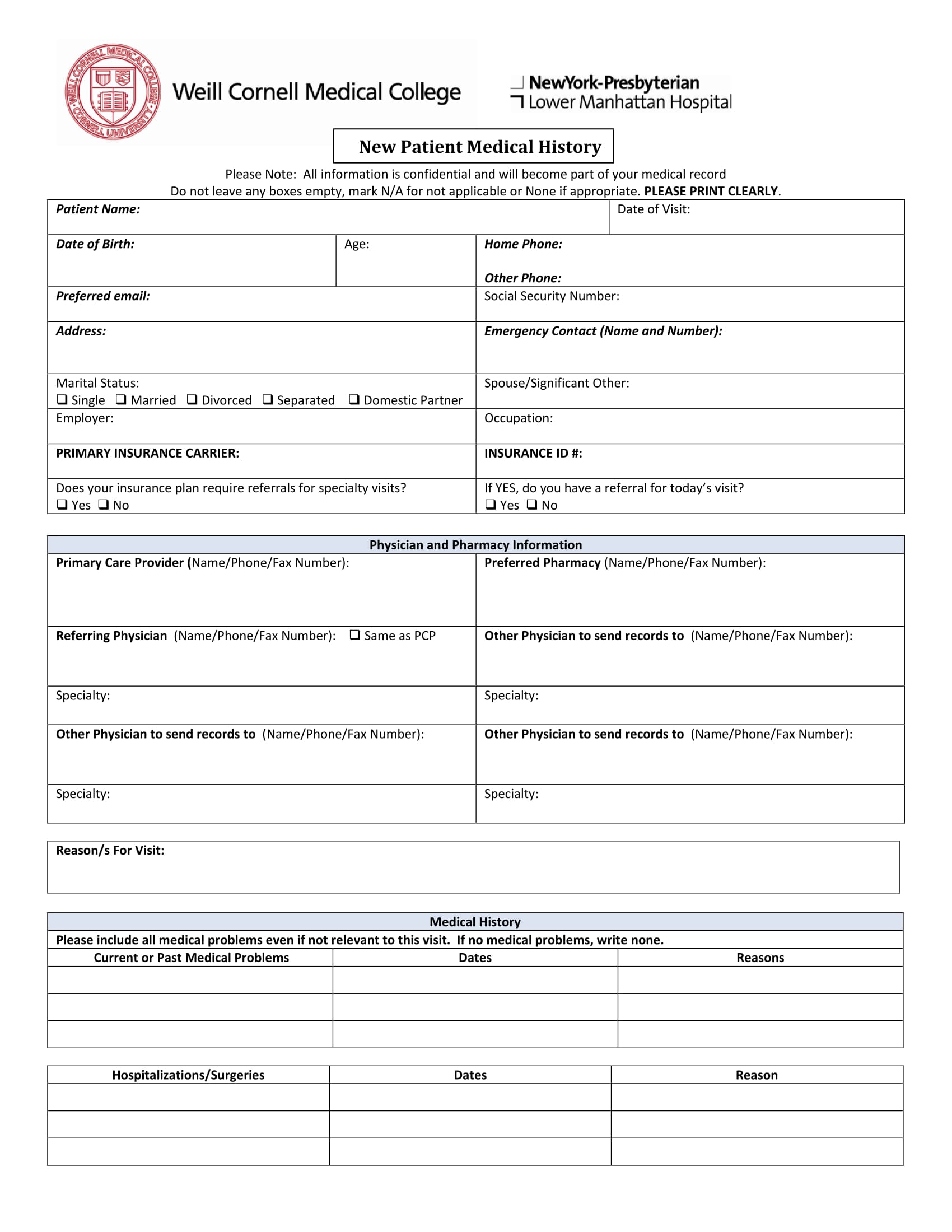
New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Have you ever been treated for any of the following medical conditions? A comprehensive form to collect personal, medical, social and quality of life information from new patients. The medical history form can help you and your patients as it provides information.
![General Medical History Forms (100 Free) [Word, PDF]](https://www.wordtemplatesonline.net/wp-content/uploads/new-patient-medical-history-form-template.jpg)
General Medical History Forms (100 Free) [Word, PDF]
New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Have you ever been treated for.
Medical History Forms 10 Free PDF Printables Printablee
New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Have you ever been treated for any of the following medical conditions? A comprehensive form to collect personal, medical, social and quality of life information from new patients. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-30.jpg)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
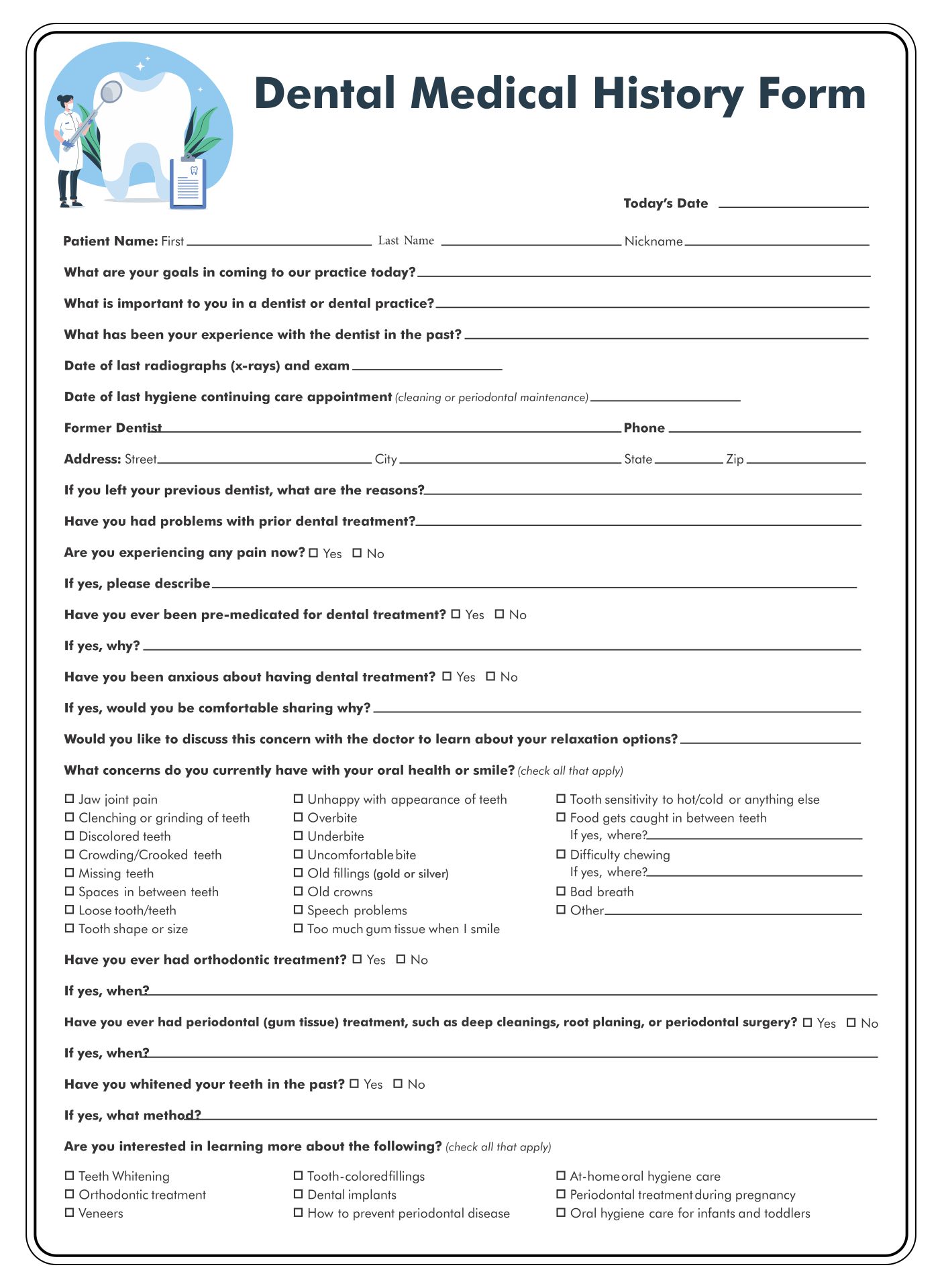
A comprehensive form to collect personal, medical, social and quality of life information from new patients. New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. Have you ever been treated for any of the following medical conditions? A pdf form to collect personal, insurance, and medical information from new.
New Patient History Form printable pdf download
The medical history form can help you and your patients as it provides information that can assist with the diagnosis, the. No changes cancer arthritis depression/anxiety please list any. Have you ever been treated for any of the following medical conditions? A comprehensive form to collect personal, medical, social and quality of life information from new patients. New patient medical.
![43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab](https://templatelab.com/wp-content/uploads/2021/02/health-history-form-09-scaled.jpg?w=790)
43 Medical Health History Forms [PDF, Word] ᐅ TemplateLab
New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if. No changes cancer arthritis depression/anxiety please list any. A comprehensive form to collect personal, medical, social and quality of life information from new patients. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal.
The Medical History Form Can Help You And Your Patients As It Provides Information That Can Assist With The Diagnosis, The.
A comprehensive form to collect personal, medical, social and quality of life information from new patients. A pdf form to collect personal, insurance, and medical information from new patients seeking surgical consultation. New patient medical history form name:_____ date of birth:_____ today’s date:_____ reason you are here:_____ personal medical history: Have you ever been treated for any of the following medical conditions?
No Changes Cancer Arthritis Depression/Anxiety Please List Any.
New patient medical history form allergy allergic reaction medications (please list all) dose times per day (mg., pill, etc.) if.