Printable Medical Clearance Form For Dental Treatment
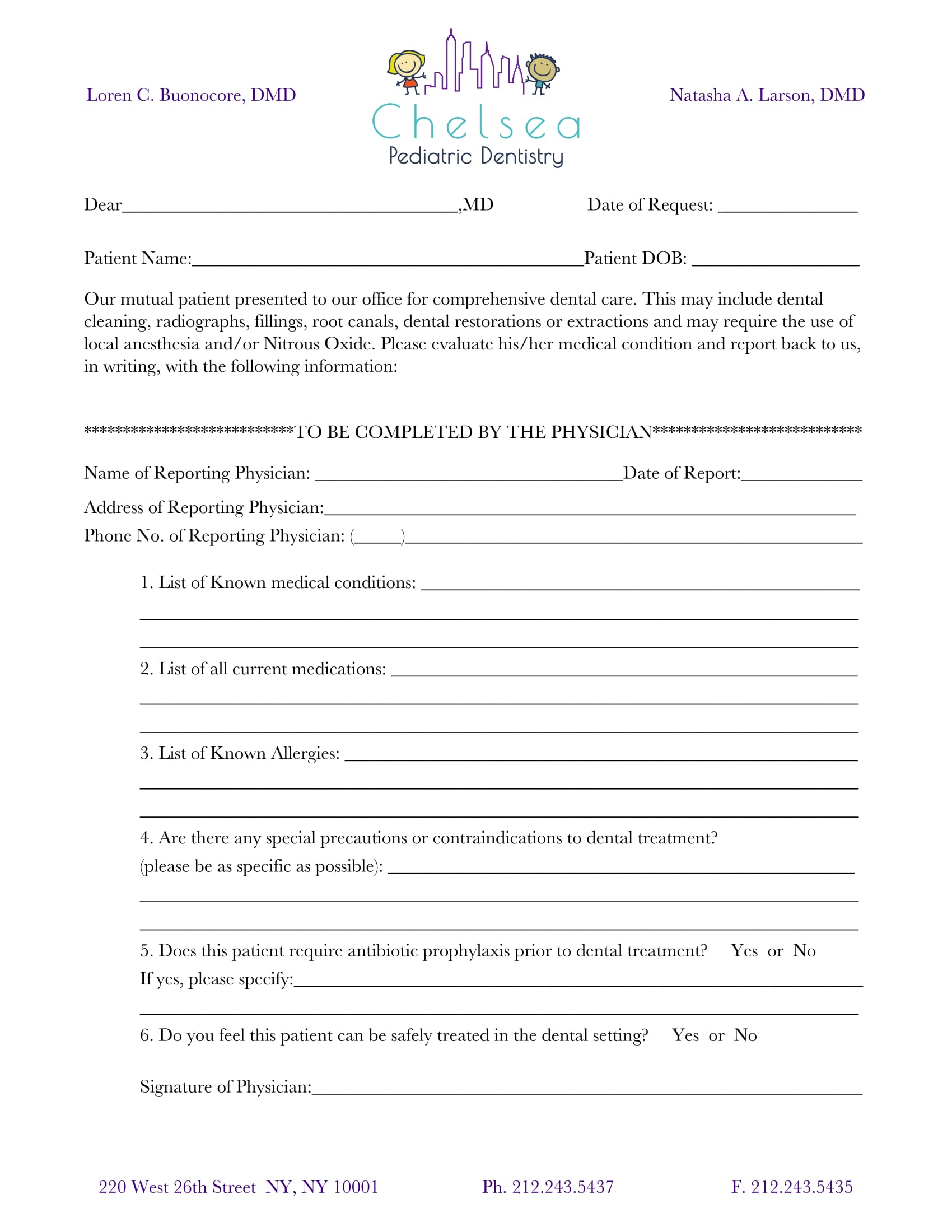
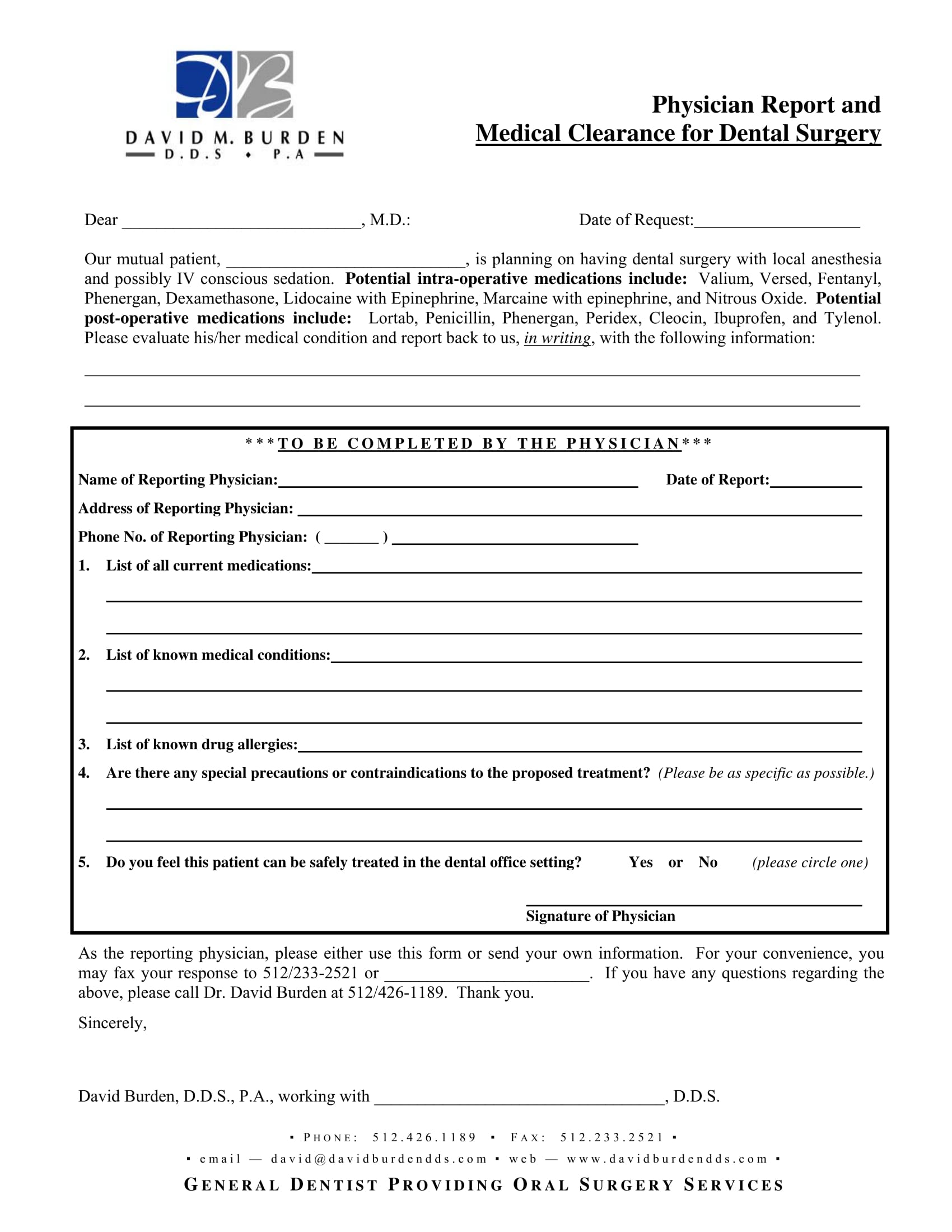
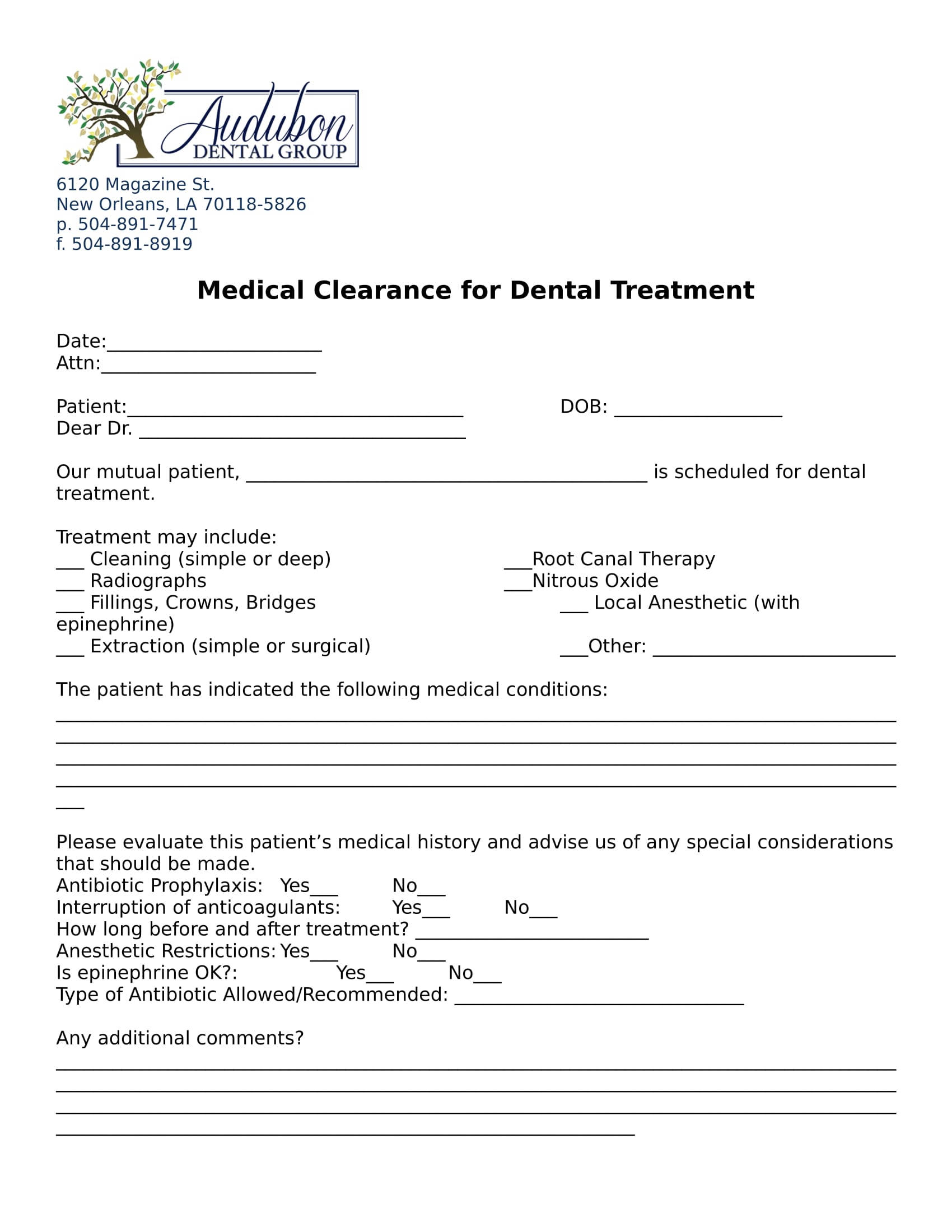
Printable Medical Clearance Form For Dental Treatment - Medical clearance for dental treatment date: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Our mutual patient, _____ is scheduled for dental treatment. The patient has indicated the following medical conditions: Dentist name (please print) patient signature date physicians:
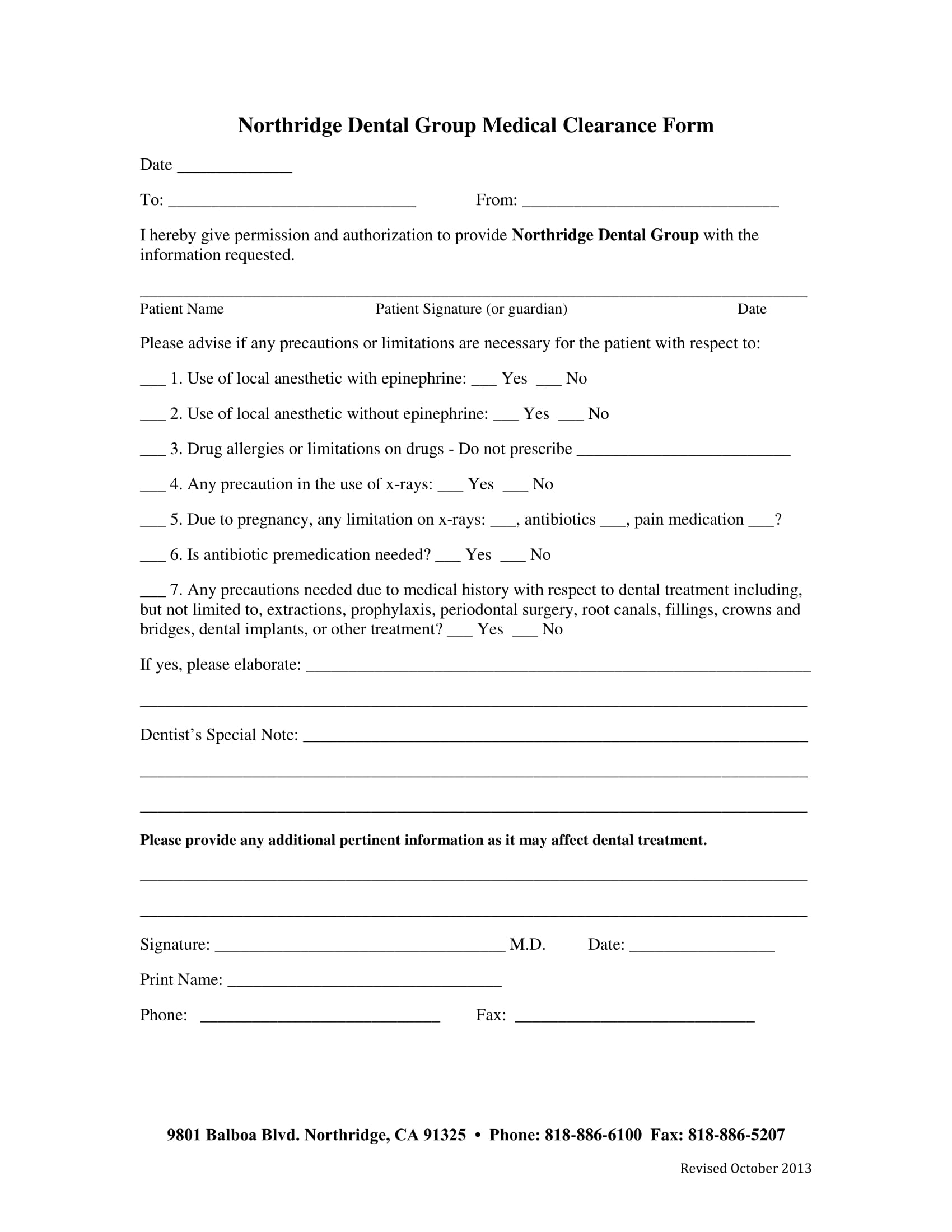
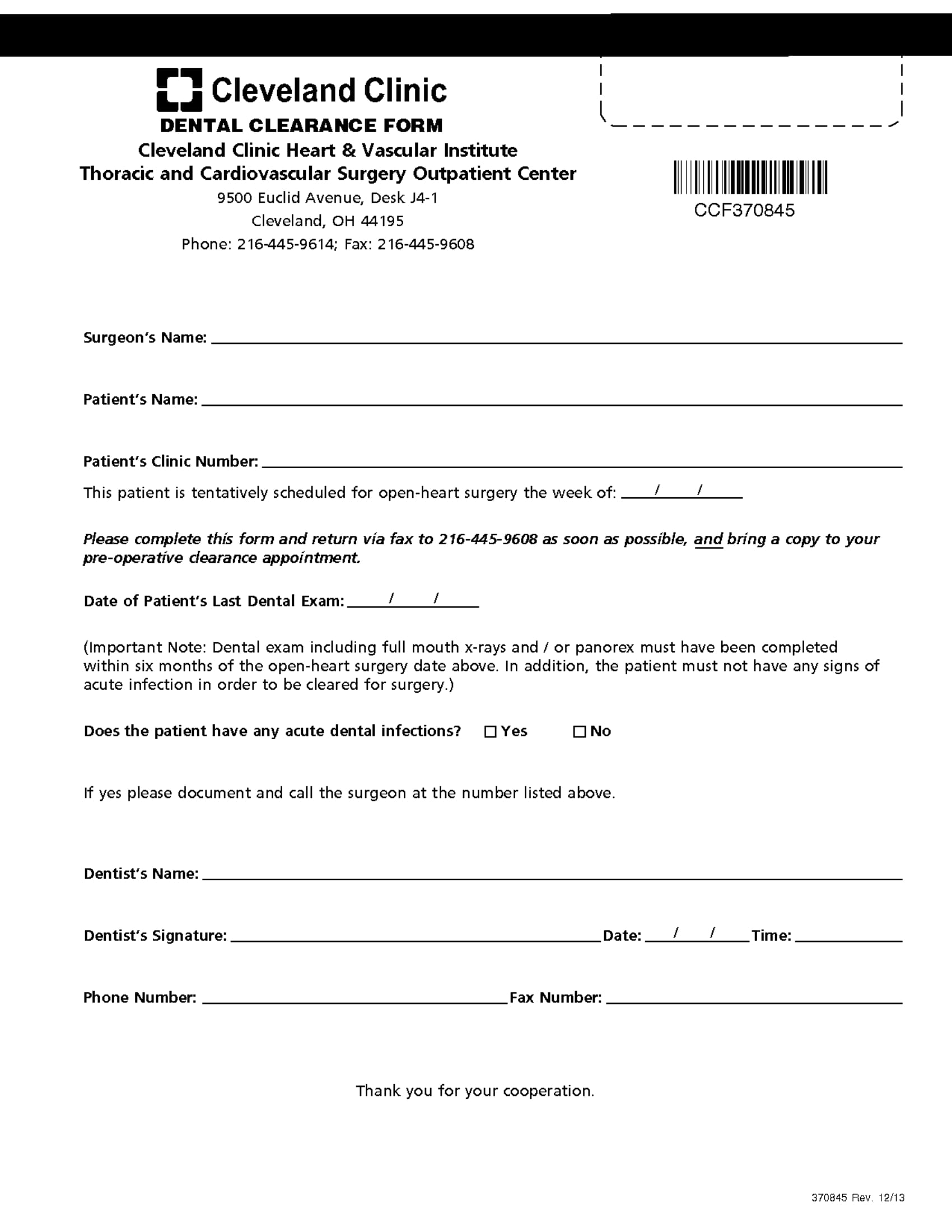
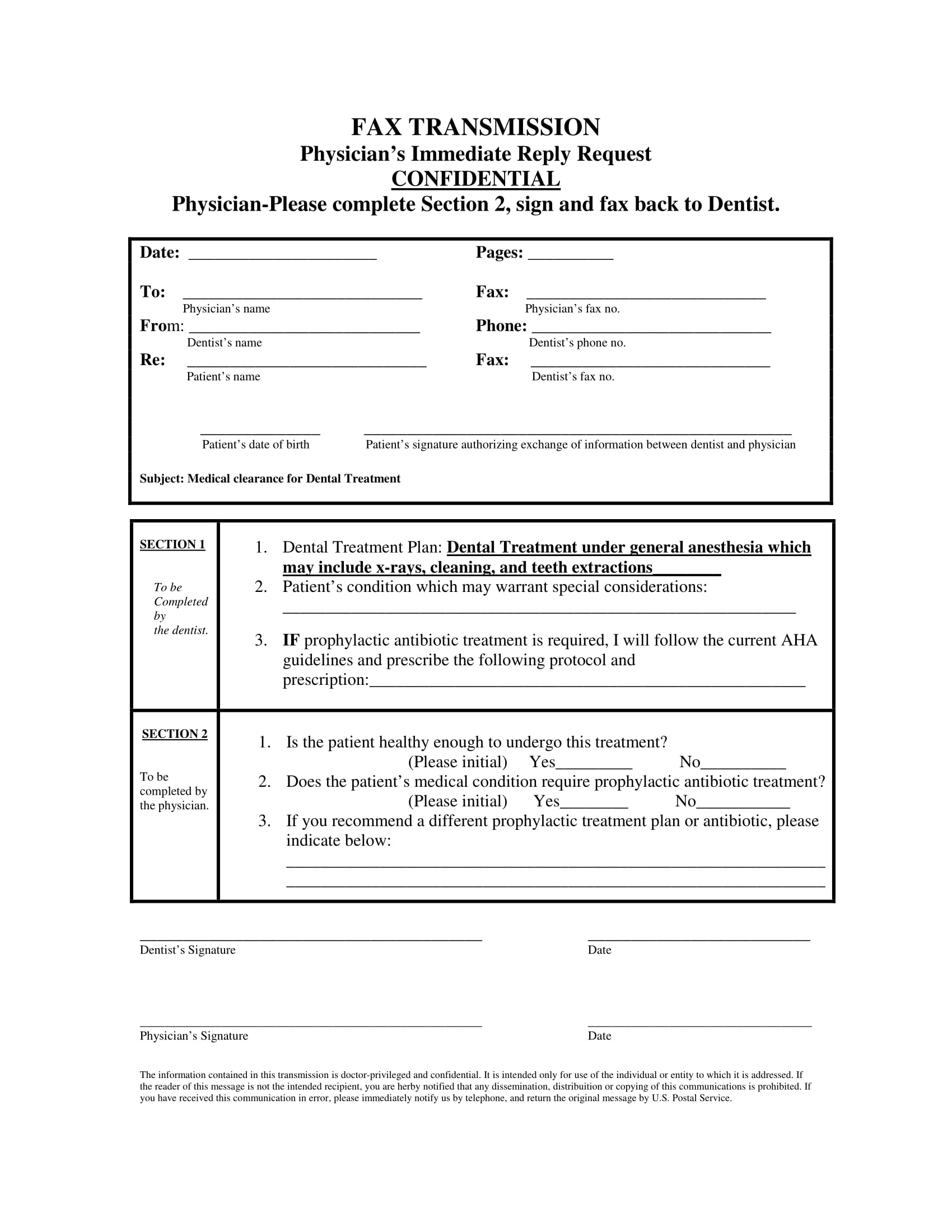
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Medical clearance for dental treatment date: Our mutual patient, _____ is scheduled for dental treatment. Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure.
Medical clearance for dental treatment date: Our mutual patient, _____ is scheduled for dental treatment. Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the.
Printable Medical Clearance Form For Dental Treatment Printable Word
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Dentist name (please print) patient signature date physicians: Our mutual patient, _____ is scheduled for dental treatment. The patient has indicated the following medical conditions: Medical clearance for dental treatment date:
Printable Medical Clearance Form For Dental Printable Forms Free Online
Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. The patient has indicated the following medical conditions: Our mutual patient, _____ is scheduled for dental treatment. Medical clearance for dental treatment date: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled.
FREE 18+ Dental Medical Clearance Form Samples, PDF, MS Word, Google Docs
Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Medical clearance for dental treatment date: Our mutual patient, _____ is scheduled for dental treatment.
Dental Medical Clearance Form Printable Printable Word Searches
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Dentist name (please print) patient signature date physicians: The patient has indicated the following medical conditions: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Medical clearance for dental treatment.
Printable Medical Clearance Form For Dental Printable Forms Free Online
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient, _____ is scheduled for dental treatment. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. The patient has indicated the following medical conditions: Dentist name (please print).
Printable Dental Clearance Form For Surgery
The patient has indicated the following medical conditions: Dentist name (please print) patient signature date physicians: Medical clearance for dental treatment date: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Our mutual patient, _____ is scheduled for dental treatment.
Printable medical clearance form for dental treatment Fill out & sign
Our mutual patient, _____ is scheduled for dental treatment. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. The patient has indicated the following medical conditions: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Medical clearance for dental.
Printable Medical Clearance Form For Dental Treatment
The patient has indicated the following medical conditions: Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Medical clearance for dental treatment date: Our mutual patient, _____ is scheduled for.

Printable Medical Clearance Form For Dental Printable Forms Free Online
Please ensure that your medical provider completes this form and returns it to your dental office before your scheduled dental procedure. Dentist name (please print) patient signature date physicians: Our mutual patient, _____ is scheduled for dental treatment. Medical clearance for dental treatment date: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation.

Printable Medical Clearance Form For Dental Treatment
The patient has indicated the following medical conditions: Medical clearance for dental treatment date: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Dentist name (please print) patient signature date physicians: Our mutual patient, _____ is scheduled for dental treatment.
Our Mutual Patient, _____ Is Scheduled For Dental Treatment.
Medical clearance for dental treatment date: The patient has indicated the following medical conditions: Please provide any information regarding the above patient's need for antibiotic prophylaxis, current cardiovascular condition, coagulation ability, the. Dentist name (please print) patient signature date physicians: